


This continues our Spring series on respiratory viruses and their complexities. Previous entries included a review of less common respiratory pathogens, and a primer on respiratory disease surveillance. Today's piece takes a closer look at how respiratory viruses spread. To support our work, consider becoming a paid subscriber.
Major routes of transmission
In the context of respiratory viruses, there are three major routes of transmission: droplet, aerosol and fomite (also known as contact). As we'll see, these are not exclusive categories. Most viruses can spread through some combination, or along a spectrum.
Droplet Transmission
Droplet transmission occurs when virus-containing respiratory particles are expelled during activities such as coughing, sneezing, or talking. These droplets are relatively large—roughly the size of visible water droplets or a grain of salt—so they fall quickly to nearby surfaces or onto the mucous membranes of people close by, particularly the nose, mouth, or eyes. Many common respiratory viruses, including influenza and RSV, are thought to spread at least partially in this way. Because the droplets don’t travel far, close contact, usually within one to two meters, is the main risk zone for transmission.
Aerosol Transmission
Aerosol transmission occurs through much smaller respiratory particles, so tiny that they are invisible to the naked eye and can remain suspended in the air for minutes to hours. These tiny particles are what most people mean when they describe a virus as “airborne.” Because aerosols are light, they can travel farther than larger droplets and accumulate in poorly ventilated indoor spaces, increasing the risk of infection even for people who are not in close contact with the infected person. Measles is a classic example of an airborne virus, because it can hang in the air for prolonged periods, even after an infectious person leaves the room. SARS-CoV-2 spreads through a combination of droplets and aerosols, with airborne particles playing a particularly important role in crowded or enclosed settings. Aerosol transmission also plays a role in the spread of influenza, with one review attributing it to half of transmission.
Contact (Fomite) Transmission
Contact transmission happens when virus is transferred onto surfaces or objects, which are then touched by someone else who transfers the virus to their eyes, nose, or mouth. These contaminated surfaces are known as fomites. Some viruses, such as rhinoviruses and adenoviruses, can survive on surfaces for hours or even days, making this route of transmission more important. Effective hand hygiene and regular cleaning of high-touch surfaces are key strategies to reduce the risk of infection through contact. While contact transmission is generally less dominant than droplets or aerosols for many respiratory viruses, it can still contribute to the spread, particularly in settings where people frequently touch shared surfaces.
Blurred Boundaries in Transmission
The distinctions between droplet and aerosol transmission are often less clear than they appear. In real-world settings, it is extremely difficult to determine exactly how a virus spreads from one person to another. Most respiratory viruses are transmitted through a combination of routes, with the relative contribution of each shaped by environmental conditions, viral load, human behavior, and susceptibility. For example, influenza may spread primarily through droplets during routine interactions, but aerosol transmission can become more important in crowded indoor environments or during medical procedures that generate fine respiratory particles, such as intubation or airway suctioning.
Transmission dynamics can also vary across viruses and populations. RSV and parainfluenza are common in young children, where close contact and shared surfaces play a larger role. In contrast, SARS-CoV-2 spreads efficiently across age groups through both short-range droplets and longer-range aerosols. Other viruses, including human metapneumovirus, adenoviruses, and rhinoviruses, fall somewhere in between, with transmission patterns that shift depending on context.
Because transmission operates along a spectrum rather than within fixed categories, prevention strategies must be layered. Measures such as masking, ventilation, hand hygiene, distancing, and vaccination each target different parts of this continuum. Their relative importance is not fixed, it changes depending on the virus, the setting, and the population at risk.
Preventing Respiratory Virus Transmission
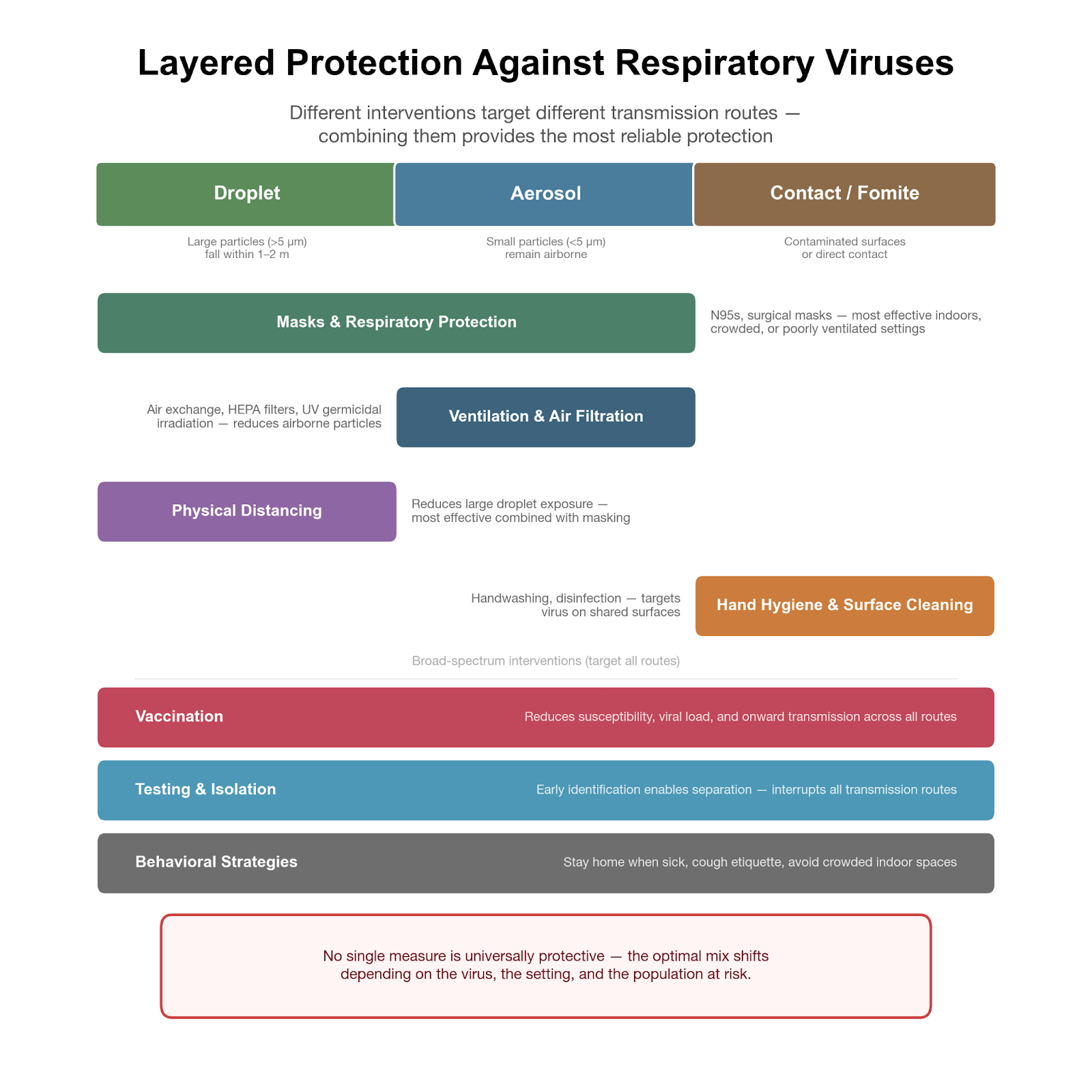
Because respiratory viruses spread along a continuum, from droplets to aerosols to contact, effective prevention requires layered strategies. Different interventions target different parts of this spectrum, and no single measure is universally protective across all settings. Instead, risk reduction comes from combining approaches that work together to interrupt transmission.
Masks and other forms of respiratory protection reduce exposure to both droplets and aerosols. Their impact is greatest in indoor, crowded, or poorly ventilated environments, where airborne particles can accumulate, and they remain particularly important for high-risk populations or during surges of viruses with risk of aerosol transmission, such as SARS-CoV-2 or measles. Ventilation and air filtration further address airborne risk by reducing the concentration of virus in shared air. Increasing outdoor air exchange, limiting recirculated air, and using high-efficiency filtration can all meaningfully lower the likelihood of inhaling infectious particles, even with modest improvements in airflow.
Physical (or “social”) distancing primarily reduces exposure to larger droplets, which tend to fall quickly and travel short distances. On its own, distancing is imperfect, but when combined with masking and improved ventilation, it adds an important layer of protection, particularly in dense indoor settings. Hand hygiene and surface cleaning target contact-mediated transmission (i.e., fomites) by reducing the chance that virus deposited on surfaces is transferred to the eyes, nose, or mouth. While this route is often less dominant for many respiratory viruses, it can still play a relevant role in certain settings, especially where shared surfaces are common like cafeterias or dorms.
Vaccination operates differently from these environmental and behavioral interventions by reducing susceptibility to infection, lowering viral loads, and decreasing the likelihood of onward transmission. Vaccines against influenza, SARS-CoV-2, RSV (for specific populations), and measles provide both individual protection and broader population-level benefits. Complementing these measures, behavioral strategies such as staying home when symptomatic, covering coughs and sneezes, and avoiding crowded indoor spaces can help to limit opportunities for transmission, particularly when the specific cause of illness is unknown. Testing and isolation add another critical layer by identifying infections early and reducing contact during the most infectious period. When used effectively, testing can guide decisions about isolation and return to normal activities, helping to break chains of transmission before they expand.
Taken together, these approaches illustrate the principle of layered protection. Because respiratory viruses can spread through multiple routes simultaneously, combining interventions provides more reliable and robust protection than any single measure alone. The optimal mix of strategies is not fixed, it shifts depending on the virus, the setting, and the population at risk.
Gage Moreno, PhD, is a genomic epidemiologist who uses large-scale sequencing data to study respiratory virus transmission, focusing on how pathogens spread through communities and how we detect them.